

Background: Sickle cell disease (SCD) is an inherited blood disorder that predisposes affected children to episodic pain events, known as the Vaso-occlusive crisis (VOC). VOC is the most common reason for emergency department (ED) visits in patients with SCD. This QI project-specific aim was to assess the meantime from check-in to first analgesic delivery to patients with VOC presenting at Holtz Children's Hospital Pediatric Emergency Department (PED) and to reduce this time by at least 20% (from 90 minutes to 72 minutes) during six months in accordance to best practice standard of care.
Methods: Standard quality improvement tools and PDSA methodology was utilized to identify root causes and countermeasures. Root cause analysis included surveys from PED staff, residents, and faculty which demonstrated a lack of practitioner familiarity with current evidence and lack of a standardized pathway.
Using this data, countermeasures were implemented, including staff education of guidelines, creation, and deployment of a readily accessible SCD VOC clinical pathway (Figure 1) for PED providers to utilize an updated electronic order set "power-plan" named PED Sickle Cell Crisis Powerplan.
A balancing measure while we attempt to reduce the time to first analgesic administration, can be an increase in workload for the nursing staff in the PED.
A PED orientation introductory email prompted residents to use our clinical SCD VOC pathway, which was also uploaded in a medical mobile app (The Hub®). We displayed point-of-care reminders, including laminated pathway cards in the PED nursing stations. Key drivers for effective pain management in the ED were identified, including a continuous reassessment of pain as well as an effective standardized pharmacological and non-pharmacological care. Institutional Board Review (IRB) approval was obtained. We recruited nursing champions to help sustain our results. Will measure the average time from triage to IV opioid dosage, to ensure IN fentanyl as drug of choice will not delay subsequent IV opioid dosage administration. PED nursing staff trained to administer IN Fentanyl to patients with a nasal mucosa atomizer, available in the Omnicell. Exclusion criteria of patients with Sickle cell disease with other ICD-10 diagnosis codes, such as acute chest syndrome, or another type of etiology for pain not associated with VOC. The main indicators were assessment-to-dose time; registration-to-discharge time; first dose-to-discharge time and rate of VOC admissions (ED/admissions). All data were collected by discrete time stamps. The database was provided by Jackson Memorial Hospital Informatics and Technology (IT) team. Data were statistically analyzed using Microsoft Office Excel 365/Prism-8. The analysis compared baseline with the first PDSA cycle from December 2019 to February 2020.
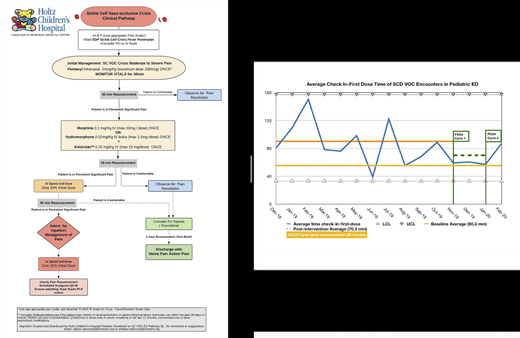
Results: From December 2019 to February 2020, a total of 65 VOC encounters were analyzed. Baseline data average check-in to first dose time was 90.3 minutes, following intervention average time lowered to 70.3 minutes, which corresponds to a 24.6% decrease (Figure 2). Patients ages 15-19 represented the majority of the participants (37.9%). Male-to-female ratio was 51.5% and 48.5%, respectively. Afro-American non-Hispanic participants represented 91.2% of the study and Hispanic 8.8%.
Discussion: PED staff surveys demonstrated a lack of familiarity with current VOC guidelines and the lack of a standardized pathway. Nursing surveys reported hesitancy to opioid re-administration from subjective pain assessment and opioid pain management misconception before education. PED staff shift changes, monthly new rotating residents, and the unpredictable nature of PED workflow are factors that can affect consistent VOC management. Implementing a clinical pathway available to the staff and integrating it into the workflow reduces the variability in the management of VOC visits. Hence, through teamwork, continuous pathway reinforcement, and education our outcome was associated with improvement in average time from check-in to first-dose.
Conclusion: Standardized procedures to treat and reassess pain for sickle cell disease VOC patients in the PED resulted in check-in to first-dose time reduction by 24.6%. Further steps to sustain our results include guideline reinforcement and interventions with effective pharmacological i.e. intranasal fentanyl and non-pharmacological care.
No relevant conflicts of interest to declare.

